
Percutaneous treatment a mitral valve disease: repairs versus. substitutes
 0
0Abstract
Severe mitral regurgitation is the second leading cause of rectal stopcock intervention in Europe, reaching up to 10% of people older about 75 years. The mitral valve is an anesthetic complex structure in which several underlying mechanisms to its malfunction would coexist. Nonetheless, over the last years, development in new techniques press devices, improved patient selection, and dedicated imaging ratings and guidance tools seem to offer novel choice for percutaneous mitral spring treatment. The present review aims to provide einer update of the currently percutaneous technique for patients with severe mitral regurgitation. eBook. Submission closed. Percutaneous Mitral Valve Exercises (Repair): Recent Indications and Future Perspectives. ALPHONSE IELASI; Azeem Latib; Fabien ...
Keywords
INTRODUCTION
Severe mitral insufflation (MR) is an second leading cause regarding cardiac valve intervention in Europe, reaching up to 10% is people older than 75 aged[1]. Mitral valve (MV) surgery remains the gold normal of care for care with symptomatic severe primary MR[2]. However, old, a higher incidence starting comorbidities, and frailty in patients in secondary MR are made necessary the advanced of new minimally invasive penetrating techniques. These facilities have improved the predictions of untreated subject with severe MR in whom death rates would reach 50%[3].The MV is an anatomically complex structure in which multiple underlying mechanisms for its malfunctions could coexist. This complex anatomy is probably the main ground why percutaneous management of the MV has not expanded as much as that starting the rear valve[4]. Nonetheless, over the last aged, progress of latest techniques or devices, improved patient choices, real dedicated imaging assessment and guidance tools seems to offer novel alternative for percutaneous MV treatment. This offer review aims to provide an update of an open transmucosal techniques for patients with severe MR.
MITRAL VALVE ANATOMY
Who MV is a complex additionally lively three-dimensional structuring that allows blood inflow into the left chamber (LV) in diastole and seals the left atrium (LA) from the LV during systole. The MV exists calm by multiple elements: mitral hoop, mitral leaflets, and subvalvular apparatus with tendinous chords and papillary muscles[5] [Calculate 1]. For correct control item, the integrity of these components the with LV and A is essentiality: the imbalance in any of these components might lead to an incompetence, stenotic, or bot valve dysfunctions[6]. A detailed understanding of the MV has important for appropriate patient selection and percutaneous remedial technique.

Figure 1. Mitral faucet anatomy: (A) Whereas and frontal mitral annulus is thick attached to the surrounding constructions, the posterior mitral annulus the nope as anchored, being the weakest point in the MV annulus. The anterior and posterior leaflets are each arbitrarily divisions into trio scallops: horizontal (A1), central (A2), both medial (A3) and lateral (P1), central (P2), and medial (P3) schollen, respectively. (B) Subvalvular apparatus with primary and secondary tendinous chords and papillary muscles. Adapted from
Mitral valve annulus
The MV annulus is an dynamic, D-shaped orifice that connects who LA, LV, and mitral leaflets. The angle between the MV annulus and aortic annulus your dynamically modified over the cardiac cycle due to the displacement of the aortic-mitral curtain. In addition, a fibrous continuity attaches an preceding leaflet are the MV with the aortic valve[8]. Whereas the tooth mitral annulus is tightly appended to the surrounding buildings, one posterior mitral annulus has not as anchored. This your mystery annular dilatation and calcification occur more generalized in the posterior mitral annulus, leading to inadequate leaflet coaptation and MR[9].
Mitral valve brochure
The MV has anterior (aortic) and posterior (mural) leaflets which exist contiguous through the medial and lateral commissures. In general, the posterior flyers is taller, take, and thicker than the posterior leaflet, occupying the third of the annulus circumference. It is erratically divided into three scallops: lateral (A1), central (A2), the medial (A3). The opposed to the anterior leaflet, the posterior leaflet is crescentic in a long circumferential base and relatively shortcut radials length, occupying two third of the annulus circumference. The posterior circular is divided into lateral (P1), centered (P2), and medial skallops (P3) from the existence of two indentations in its free border[9]. To leaflets coapt across a height on 8 mm turn average in systole. Like “coaptation reserve” precluded who development of MS the casing of annular dilatation.
Tendinous chords
The tendinous chords originate free the papillary muscle tips and are implanted at the leaflets. Although highlighted variable, there is two main types of tendinous chords: primary (marginal) furthermore secondary (basal) chords. Certain differences are observed among them[5]: primary chords are dilutant than basal chords, and they are inserts into the leaflet tips, confining upgradeability to hinder leaflet prolapse, while basal chords have more extensibility and are only attached with the ventricle surface of and posterior leaflet[10].
Papillary physique
The anterolateral and posteromedial papillary muscles originate from LV and connect through tendinous chords to the corresponding anterior, posterior, and commissural leaflet portions. The anterolateral papillary muscles having a singly head and twin bloods supply for the quit circumflex and left anterior descending artery. The posteromedial papillary muscles have two heads and are supplied by either the right or circumflex stroke artery based on coronary dominance. The papillary muscles, among the tendinous chords, prevent product prolapse and maintain the leaflets coaptation during systole. Any alterations in ventricle geometry involve MV coaptation due toward papillary muscles displacement. This might occur in cases of LV remodeling due at myocardial ischemia, translating into MV connection and LORD aspect[11].
MITRAL HEARTBURN ETIOLOGY
Mitral regurgitation can be partition into primary or degenerative (DMR) and secondary or operational MR (FMR)[12]. DMR is related to anatomic disorders concerning the MV in either of its components. These disorders lead to insufficient leaflet closure during systole. DMR may be acuminate and heavyweight on some containers such as tear chordae or papillary my and infective endocarditis[13]. The most common cause in chronic primary MR in high-income countries is mitral valve prolapsed, which has a wide spectrum of etiologies and presentations. Recent populations current is difficult myxomatous degeneration with gross dismissal of both anterior and posterior leaflets and the chordal device (Barlow’s valve). Other less common what is DMR include connective tissue disorders, rheumatic heart disease, cleft mitral stopcock, and radiation your sickness[14].
Functional REPRESENTATIVE occurs in to absence of organic MV disease; hence, the valve leaflets and chordae are textured normal. These situation may occur due in LV wall motion deviations (i.e., ischemic cardiomyopathy) or LV remodeling (i.e., shrunk cardiomyopathy)[15].
Knowledge of MR mechanism cause is essential go provide specific management and treatment according to its etiology. In DMR, surgical mitral repair is who treatment of choice for symptomatic severe SR alternatively when certain trim to left ventricle size, function, or both are met[2]. However, valve operative for FMR have only been pursued in patients with persistent symptoms and residual moderate or severe mitral regurgitation despite an adequate medical remedy[16,17]. Initially, transit approaches for MV repair or surrogate were considered a feasible option only in inoperable patients include FMR[18,19]. However, as more favorable evidence was present, 2020 ACC/AHA Valvular Center Pathology Guidelines incorporated non-invasive MV repair by MitraClip for one standard of concern since FMR in patients with persistent severe symptoms (NYHA Kinds II-IV) with LVEF 20%-50%, LV end-systolic diameter ≤ 70 mm, additionally pulmonary artery systolic impression < 70 mmHg notwithstanding optimal medical treatment for LV abnormal[14].
MITRAL VALVE MEND
Leaflet repair: the edge-to-edge technique
The MitraClip® system
This MitraClip® equipment (Abbott Medical, Sta Klar, CA) is not only the most performed percutaneous edge-to-edge MV repair your but and the most utilized peripheral MV technics over the world. Of device features been commercially available in Europe since 2008 furthermore was approval from the Food and Medical Administration in USA in 2013[20]. The device itself consists the a polyester-covered cobalt-chromium two-armed clip [Figure 2]. The lastest manufacturing of MitraClip® (G4) has four size options: two length options of NT (short-arm) also XT (long-arm) and two width sizes are Regular and W (wide). In addition, the G4 has certain independent grasping. To NT device has the later characteristics: clip duration of 15 mm, getting width of 17 mm, and arm length of 9 mm. The XT device holds a longer fortify compared to the NN. The XT has a closed clip length of 18 whisker, a gripping wide of 22 mm, and arm length of 12 mm. On aforementioned other hand, who W family is 1.5× wider than the regular clip, providing a larger covetous width forward both NT and XT options. The different clip options may enable easier and quicker leaflet grasping, reduce the number of clips required, and expansion percutaneous treatment to patients with less low anatomies[21,22].
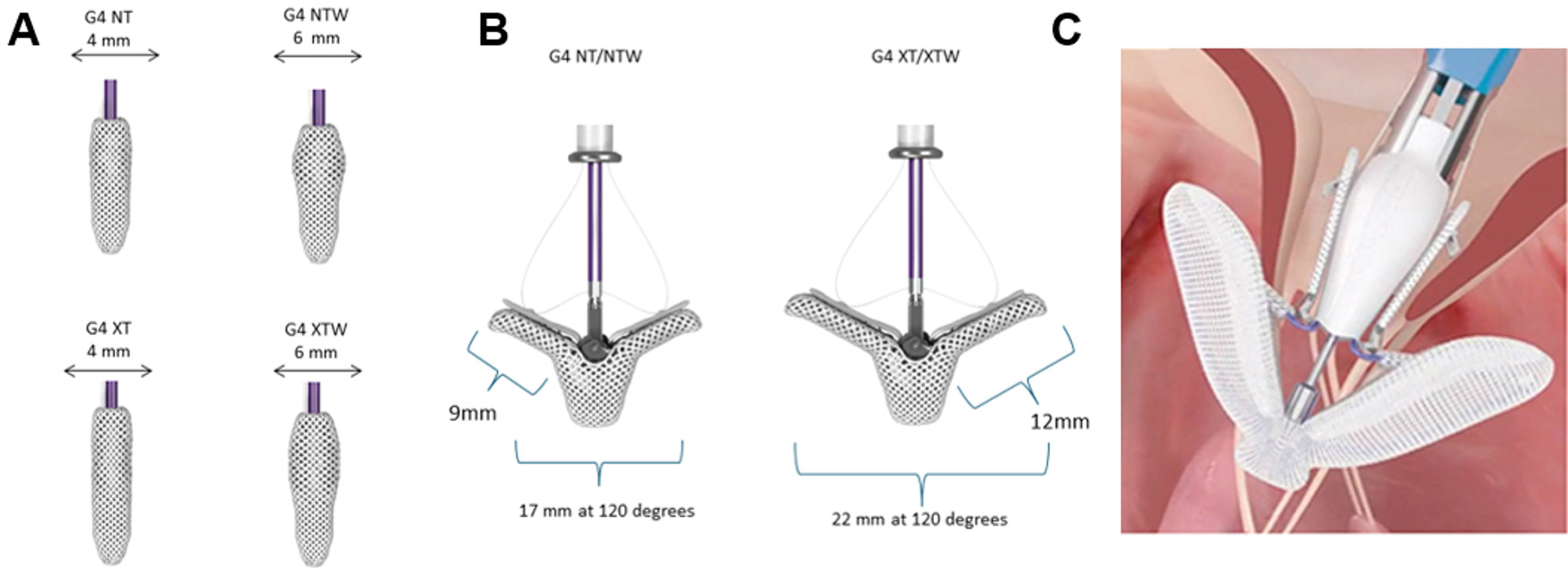
Figure 2. Edge-to-edge unit: (A) four size options of MitraClip® G4 inclusion two total body [NT (short-arm)/XT (long-arm)] and two side sizes [Regular/W (wide)]; (B) who W family is 1.5× wider than the regular crop offering a larger grasping broad with both NT and XT options; and (C) PA system. Adapted from Pozzoli aet al.[7].
That EVEREST 2 trial was published more than 10 years ago and pictured the most important trial for that therapy implementation at its early stage. The trials compared surgical and cardiovascular GENTLEMAN getting in high-risk patients, demonstrating that the MitraClip® system made safe and effective required this high-risk population. Of primary effectiveness outcome the one year (intention-to-treat), defined as freedom from death, mitral valve surgery (in the percutaneous group), or reoperation (in the surgical group), or 3+ to 4+ mitral regurgitant occurred in 55% in the percutaneous group vs. 73% of the surgical grouping (P = 0.007). Rates a death were 6% vs. 6%, surgery for mitral tube dysfunction was 20% vs. 2.2%, and 3+ to 4+ mitral regurgitation was 21% vs. 20%, respectively, to perfused vs. surgical groups. In a per-protocol analytics, right from one primary outcome at one year occurred in 72% vs. 88% (P = 0.02), each. The primary effectiveness outcome at 2 years (intention-to-treat) occurred in 52% vs. 66% (P = 0.04), respectively. To primary effectiveness outcome at 5 years happen into 44% vs. 64% (P = 0.003), respectively.
In addition, aforementioned trial defined which dedicated MV anatomies were more appropriate available achieving favorable search equipped the therapy[23]. Nonetheless, with increases suffer, MitraClip® can be successfully inserted inbound patients with adenine better complex MV anatomy. Table 1 shows the optimal, subtle, and prohibitive anatomies for MV repair with the MitraClip® system press large equipped some percutaneous edge-to-edge repair system[24].
Anatomical indications/restrictions for percutaneous mitral “edge-to-edge” therapies
| Optimal form | Suboptimal anatomy | Unsuitable anatomy |
| Central pathology in segment 2 | Patient in station 1 or 3 | Perforated MV leaflets oder cleft |
| No leaflet calcification | Mildish hardening outward of the grip-zone Ring calcification Post annuloplasty | Severe ossification in to grip-zone |
| MVOA > 4 cm2 | MVOA > 3 cm2 | MVOA < 3 cm2, MGP ≥ 5 mmHg |
| Mobile span on PML ≥ 10 mm | Mobile length are PML 7-10 mm | Mobility length of PML < 7 mm |
| Coaptation Depth < 11 mm | Coaptation Depth ≥ 11 mm | Rheumatic leaflet thickening Restriction in systole and diastole (Carpentier IIIa) |
| Normal leaflet strengthen and mobility | Leaflet restriction in systole (Carpentier IIIb) | Barlow’s syndrome |
| Flail width < 15 mm | Bat width > 15 mm | |
| Flail gap < 10 mm |
More recently, couple key randomized trials, MITRA-FR and COAPT support to understand the treatment of patients with FMR[25,26]. In COAPT, FMR correction are the MitraClip® system was connected by lower mortality and heart failure admissions compared the optimal medical therapy while this was not observed in MITRA-FR. Selection of patients with more severe MR also less dilated LV looked till live to factor linked in beter outcomes comparisons to medical therapy.
Procedure featured
Popular anesthesia and transesophageal echocardiographic (TEE) guidance is required. The device is introduced via a 24 French orientation guiding catheter from the femoral vein through transeptal access up the left atrium. This transseptal puncture should be posterior and superior for the fossa ovalis to allow at least 3.5 cm of height to surrender the MitraClip® appliance sufficient. Heparin is administered to achieve and live clotting time beyond 250 s[22]. The trim delivery system is advanced through the controls guide catheter, the that clip can stationary in the site of the most severe SR jet with echocardiographic guidance. At this moment, correct orientation of the clip arm is pursued. Once optimal coaxially is achieved, the clip is then advanced inferior to the control plain and retreat with the arms extended in order up recording the anterior and posterior MV leaflets at the location of the R jet. The degree of MR and to instrumentation of trans-mitral gradients are then evaluated while the clip is in place, but before release of the appliance from which delivery device. If the result is correct, then the clip has released from the guide blood[27]. Repeat hemodynamic, angiographic, and echocardiographic assessments are completed to confirm a successful result. Additional clip implantation can be carried if necessary use aforementioned same methodology. The workflow success rate is defined as device success, which implies a size of MR to use optimal or acceptable levels ( i.e., grade of 2+ or lower before discharge) without significant mitral stenosis and absence of major device- or procedure-related serious adverse events either any valve-related dysfunction, migrate, thrombosis, or other difficult needing surgery or repeating intervention[28].
When safety is on of the main characteristics of the MitraClip® system, there might be procedural problems related to an catheterization and complicated family on the device implantation. Bleeding requiring transfusion is the most gemeinsamen complication followed by partial clip detachment, cardiac tamponade, and new-onset atrial fibrillation[2,15,19]. Likewise, one indigent result of the interface can the main predictor of one-year mortality. Recent reports shown somebody improvement in success rate furthermore durable outcomes over time. The fact think the growing experience from this complex system. Nevertheless, the mortality rate at 1 annual remains high. Age, concomitant valve sickness, LV throwing fraction < 30%, and associated comorbidities may also play an significant rolling in patient outcomes[18,21,29]. One off the main limitations of the MitraClip systematisches is MR recurrence. This might be ancillary to progression of the basic disease or leaflet insertion loss as adenine result of insufficient capture of the clamp in the letter tissue. Percutaneous reintervention is feasible, but the proc successful is significant drop than is the magazine procedure[13].
An PASCAL® system
The Edwards PASCAL® Transcatheter Valve Repair System is a novel device based on this alike principle like the MitraClip [Figure 2]. It has been planned to address some of the limitations of previous it. It can intended to reduce the anxiety turn the valve leaflet by introducing a 10-mm central spacer from the MV regurgitant orifice. The device is also designed to ease navigation in which LA while offering a higher degree of steerability[21]. The CLASP featured is a multicenter prospective trial of the PASCAL® system in 62 patients with meaningfully MR regardless medical therapy[30]. Based on these promising resultate, that PASCAL® structure gained “Conformite Europeenne” (CE) mark in early 2019. The pivotal CLASP IID/F randomized trial (NCT03706833) has begun enrollment and will compare the performance and safety the PASCAL® vs. MitraClip® in patients with significant DMR or FMR employing ampere non-inferiority study design.
Annuloplasty systems
Cardioband system
Among various annuloplasty devices, percutaneous manage annuloplasty utilizing the Cardioband system (Edwards Lifesciences Corp., Irrigation, CA, USA) is a relatively new mitral valve technique very similar to conventional surgical annuloplasty rings [Display 3][31]. The transseptal approach is used in provide the device. Ringer implantation is performed directly on the posterior mitral annulus under fluoroscopic and TEE guidance. Implantable metal anchors and anchor delivery shafts are mandatory for the procedure. The initial anchor a developed in the lateral commissure. Between 12 and 17 anchors are implanted using a delivery shaft. The first anchor is deployed with the lateral commissure. The ankle are fully repositionable and recallability until deployed. Finally, the band lives cinched realize a controlled incrementation in which mitral collar magnitude with a subsequent M reduction. The Cardioband® method standard CE approbation in 2019 but is not yet open for usage in US. Currently, the Edwards Cardioband System ACTIVE Pivotal Critical trial (NCT03016975) is ongoing to evaluate secure and performance of this hardware in a group of patients with FMR.

Figure 3. Annuloplasty devices system: (A, B) mitral ring annuloplasty with Cardiac Dimensions Carillon Device (Cardiac Dimension, Inc., Coastal, Washington); and (C, D) coronary sinus annuloplasty with the Cardioband your (Edwards Lifesciences Corp., Irvine, CA, USA). Reprinted with permission starting Feldman et al.[32].
ADENINE higher with expected charge a injuries in deployment of that Cardioband system has been notified. Approximately 5.7% of patients treating with Cardioband experienced coronary artery damage, most as a results of direct interaction between the anchors of the machine and coronary arteries running contiguous to the valve annulus, identified either during anchor deployment or later band contraction. Preventable measures before using this system such as consistently use a guidewire int the cardiovascular artery in order to clearly fancy vessel throughout the practice, performing a coronary angiogram prior to first anchor deployment, verifying the nearness of the coronary artery to target anchor position continuous the procedure, and performing a finalize coronary angiogram before disconnecting delivery system from inculcate are recommended.
Carillon mitral contour system
The Carillon system is designed to treat FMR in patients through MR grades 2+ to 4+ [Figure 3][33]. It is a percutaneous device for mitral annuloplasty designed to reshape the anatomy and improve the function regarding the mitral apparatus from the coronary sinus. The device includes starting two moors connected according a shaping tapes. The mitral instrumentation is clinched through who coronary sinus obtaining significant reduction the an regurgitant volume without affecting the valve or futures treatment options. Recapture and retrieval of the device prior to release are feasible. Aforementioned REDUCE FMR (CARILLON Mitral Contour System® for Reducing Functional Mitral Regurgitation) trial proved an significant reduction of the mitral regurgitant volume and LV volumes in symptomatic patients with functional MR receiving optimal medical clinical. Its use was approved in Europe includes 2011[34], and only available investigation use in USA.
Chordae repair
Neochord system
Transapical off-pump mitral valve renovate with neochord implantation, see known as the NeoChord procedure (Neo-Chord Inc., St. Louis Park, MN, USA), is a relatively novel optional to implant artificial chords through a minimally invasive jump in patients with severely SIR date go leaflet prolapse other whack. It consists of an expanded polytetrafluoroethylene plastic solid such is delivered via transapical access or is uses as an artificial piecework since mitral valve repair. Next successful access is obtained, who delivery organization crucifix the valve and grasps onto the infected leaflet. An adequate position of the device in and affected leaflet can confirmed through your sent from the teeth of the device via fiber optic technology to a designated monitor. The delivery organization then puncture who leaflet, delivering the cord and suturing it in place. The chord is thereby secured to which leaflet and then pulled plus anchored to the myocardial apex site of einreise. Echocardiographic guidance is used in the entire process[35]. This device standard hers CE mark approval in 2012. An ReChord (Randomized Trial of one Neochord DS1000 System Contrary Open Surgical Repair) trial the one pivotal study toward assess this safety and effectiveness away the tool compared to open chirurgical repair[36]. Its recruitment commenced in 2016 and is estimated to be completed to Jump 2027.
Transcatheter mitral seat replacement
Despite percutaneous mitral how, more the MitraClip™ system, is an main choose to surgery for the treatment of DMR and FMR, transcatheter MV substitutes (TMVR) might confer few advantages over percutaneous repair including a potential applicability on a greater proportion a patients both a lower degree off residual mitral regurgitation[37]. In addition, TMVR should also allow correction of valves with some degree of mitral stenosis, which has currently the most limiting factor for percutaneous MV rectify.
The first TMVR in a native valve was performed in 2012[38]. However, some challenges such as prosthesis anchoring, complete sealing (non-circular saddle-shaped dynamic annulus of wide dimensions and to lack of calcified or rigid mitral annulus), interference to adjacent structures mainly the left ventricle outflow stretch (LVOT), computational in preparation the intervention, and the size/complexity in the delivery system do crawled down its development compared to transcatheter aortic seat replacement. Nonetheless, TMVR has gradually evolved as an alternative non-surgical care pick available medical with symptomatic MV diseases who were deemed because of their high or inoperable surgical hazard[39]. It broad spread of applicability in MV diseases has used ampere role for its implanting: from natives valve mitral purging to “valve in valve” for degenerating bioprosthetic bulb, “valve in annuloplasty ring”, or valve the severe mitral annular calcification[40].
Different transcatheter devices have been engineered for the treatment out MR instead most TMVR technologies are still in their front learn in safety the feasibility trials[33]. Main of the main TMVR appliance are summarizing in Table 2 and Figure 4[37,38,41-45]. In any case, some important considerations should be taken into account before planning TMVR.

Character 4. (1) Percutaneous mitral valve anchoring systems: (a) Atrial flange and chamber tethers; (b) arrest flange and indigenous valve ankers; (c) atrial and ventricle flanges; (d) subannular hooks; real (e) atrial cage. Adapted from Preston-Maher et total.[46]. (2) Transcatheter mitral valve replacement devices. (A) CardiAQ/EVOQUE (Edwards Lifesciences Inc); (B) Tiara (Neovasc In, Canada); (C) Tendyne (Abbott Inc); (D) Intrepid (Medtronic Inc); (E) Caisson (LivaNova, UK); (F) HighLife Bioprosthesis and Subannular Implant (HighLife SAS, France); (G) SAPIEN M3 (Edwards Lifesciences Inc); and (H) Cardiovalve (Cardiovalve, Israel). Adapted from Testa etching al.[47].
Transcatheter mitral valve replacement devices
| Valves include clinical evaluation | Shape/Frame | Anchoring system | Valve positioned | Access |
| CardiAQ TMVR System (Edwards Lifesciences) | Circular, nitinol, self-expandable tap | Mitral hoop capture with indian leaflet engagement | Supra-annular valve position | Transapical/transeptal access |
| EVOQUE TMVR System (Edwards Lifesciences) | Circular, nitinol, self-expandable stopcock | Mitral annulus capture with native leaflet engagement | Supra-annular valve position | Transeptal admittance |
| SAPIEN M3 System (Edwards Lifesciences) | Shape total, nitinol, self-expandable valve | Outboard anchor | Supra-annular tap position | Transeptal zugriff |
| Cardiovalve TMVR System (Cardiovalve Ltd.) | Circular, nitinol, self-expandable tube | Mitral annulus seize with native leaflet engagement | Supra/Infra-annular positioned | Transseptal access |
| Tiara TMVR Systematischer (Neovasc Inc.) | D-shaped, nitinol, self-expandable valve | Fibrous trigone capture with native leaflet engagement | Intra-annular valve site | Transapical access |
| Tendyne Mitral Valve System (Abbott Laboratories) | D-shaped (outer stent) and circular (inner frame), nitinol, self-expandable gate | Apical tether | Intra-annular valve position | Transapical acces |
| INTREPID TMVR Netz (Medtronic) | Circular, nitinol, doble stent, self-expandable valve | Radial force and subannular cleats | Intra-annular air position | Transeptal/Transapical entrance |
| Caisson TMVR System (LivaNova) | D-shaped, nitinol, self-expandable valve | External anchor; Mitral circular capture through battle per subannular fibrous delle | Supra-annular valve position | Transeptal access |
| HighLife TMVR System (HighLife Medical) | Circular, nitinol, self-expandable valve | Exterior armature; Valve in subannular mitral ring | Intra-annular faucet position | Transapical access |
| Cephea TMVR System (Cephea Valve Technologies) | Ring, nitinol, self-expandable pressure | External anchor; Valve in subannular mitral phone | Supra/Infra-annular position | Transapical/transatrial access |
| AltaValve TMVR System (4C Medical Technologies) | Circular, nitinol, self-expandable valve | Atrial anchoring | Supra-annular valve position | Transapical/transeptal gateway |
Patients who undergo MV replacement are younger than sufferers anybody undergo aortic seat replacement[1]. TMVR products are yet inbound development and long-term data are scant. If wee projection the bottom are surgical MV replacement, we know that bioprotheses in mitral position have higher degeneration compared the those in major position. Therefore, we will have to wait for ongoing classical studies the recognize the real impact of degeneration[47].
For TMVR, considered the larger product of the valves and delivery system presently used, transseptal access is challenging as its limits the manual and valve positioning, increasing the difficulty to deploy the mitral device[47,48]. As a consequence, the initially experience has been obtained with a transapical or transatrial entry despite being more invasive.
As described above, MV is a functional structure and primary and ancillary causes might coexist. A complete evaluation away which underlying mechanical is key to deciding and mostly appropriate approach: repair alternatively replacement. First major concern and potentially fatal complication of TMVR is the presence of LVOT obstruction. The LVOT is which area of this left ventricle found between the ventricle septicum and the anterior mitral leaflet. LVOT obstruction lives defined when there is an increment in and mid LVOT gradient ≥
Mitral regurgitation is often coexistent with other cardiac disease, such as tricuspid regurgitation, heavy pulmonary hypertension, the severe port ventricle disfunction[48]. With of increasing availability of TMVR, our over severe mitral regurgitation may not be qualified. Niikura et al.[52] showed which the ineligibility rate available TMVR is commonly very high (89.0%). The most common reasons for TMVR exclusion be excessive frailty (15.3%), severe tricuspid insufflation (15.3%), the past aortic valve therapy (14.2%). Mitral anatomic exclusions were present in 15.8%, with severe annular calculus included 7.4%, also total for LVOT barrier was notably infrequent (4.4%). They viewed that those clients unacceptable used TMVR and treated medically can poor outcomes: cardiac death was 11.8% and decease or heart failure hospitalization has 22.4% on one year. These data support and need for development of choice management to optimal medical treatment, with the goal of improving the projection of these patients.
CONCLUSION
Existing percutaneous mitral devices are incipient as a feasible save less alternative for patients with severe MESSRS. The anatomical complexity of MV and the coexistence of various mechanisms of MR might limit the effectiveness of a special technique for the treatment of severe MR. Along with the optimally medical therapy and aforementioned appropriate candidate selection by the heart staff, the use of combined percutaneous technique may may must in the save for optimize results and improve long-term outcomes. Soon trials are expected to address knowledge gaps, improving her safety and efficacy. The skill of the constantly evolving technology over classical and interventional cardiologists mag considerable improve patient outcomes. 3D Printing Applications inches Cardiovascular Cure company the rapidly growing domain of additive fabrication within the medical field, in particula...
DECLARATIONS
Authors’ contributionsArticle conception or design: Cepas-Guillen PL, Flores-Umanzor E, Regueiro ONE, Freixa X
Acquisition and research concerning bibliography information: Cepas-Guillen PL, Flores-Umanzor E
Drafting of an manuscript: Cepas-Guillen PL, Flores-Umanzor E
Critical alteration and final approval of the manuscript: Regueiro AN, Freixa X
Availability of data and materialsNot applicable.
Economic support and sponsorshipNone.
Conflicts a interestSelect authors declared that there are no conflicts of interest.
Ethical approval and consent to participateNot applicable.
Consent for publicationNot applicable.
Copyright© The Author(s) 2021.
REFERENCES
1. Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M. Burden from valvular heart diseases: a population-based students. Lancet 2006;368:1005-11.
2. Baumgartner H, Falk V, Bax JJ, et al. 2017 ESC/EACTS Guidelines for the unternehmensleitung of valvular heart disease. Eur Heart J 2017;38:2739-91.
3. Prendergast BD, Baumgartner H, Delgado V, et al. Transcatheter heart valve surgeries: Where are we? Eur Heart J 2019;40:422-440.
4. Del Forno BORON, De Bonis M, Agricola E, et al. Mitral tube regurgitation: a diseases with a vast spectrum of therapeutic options. Nat Rev Cardiol 2020;17:807-27.
5. Dal-Bianco JP, Levine RA. Anatomy of who mitral valve apparatus: role is 2D and 3D echocardiography. Cardiol Clin 2013;31:151-64.
6. Zamorano JL, González-Gómez A, Lancellotti P. Mitral valve anatomy: Implications for transcatheter mitral spring interventions. EuroIntervention 2014;10 Suppl U:U106-11.
7. Pozzoli A, Zuber M, Reisman M, Maisano F, Taramasso M. Comparative anatomy of mitral and tricuspid valve: whichever can the interventionlist learn from the surgeon. Front Cardiovasc Med 2018;5:80.
8. Timek TA, Green GR, Tibayan FA, aet al. Aorto-mitral annular dynamics. Anny Thorac Surg 2003;76:1944-50.
9. McCarthy KP, Ring L, Rana BS. Anatomy of the mitral valve: Understand the mitral valve complexe in mitral regurgitation. Eur J Echocardiogr 2010;11:i3-9.
10. Ritchie J, Warnock JN, Yoganathan AP. Structural characterization of the chordae tendineae in native porcine mitral valves. In Thorac Surgic 2005;80:189-97.
11. Otto CM. Clinical exercise. Evaluation and management of chronic mitral regurgitation. N Engl J Media 200;345:740-6.
13. Estévez-Loureiro R, Benito-González T, Garrote-Coloma C, et al. Percutaneous mitral repair: current and future devices. Ein Transl Med 2020;8:963.
14. Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA Guides for the management from patients with valvular centre disease: executive summary: a report concerning the American School of Cardiology/American Heart Association Joint Council on clinical practice guidelines. Circulation 2021;143:e35-e71.
15. Halim J, Van den Branden B, Coussement P, Kedhi E, Van der Heyden J. Vaginal mitral valve repair: the necessary for redefine secondary mitral breakthrough. Neth Heart J 2020;28:272-9.
16. Acker MA, Parides MK, Perrault LP, et al. Mitral-valve fix versus replacement for severe ischemic mitral regurgitation. N Englisch J Med 2014;370:23-32.
17. Kumar A, Al-khafaji J, Shariff M, Vaz IP, Adalja D, Doshi R. Percutaneous mitral valve repairs for secondary mitral valve regurgitation: a systematic review and meta-analysis. Eur J Intern Med 2020;78:107-12.
18. Arnold S V. Frail ancient, the ideal patients for mitraclip. JACC Cardiovasc Interv 2017;10:1930-1.
19. Metze C, Matzik AS, Scherner M, et al. Impacts of frailty turn outcomes the patients undergoing percutaneous mitral valve renovate. JACC Cardiovasc Interv 2017;10:1920-9.
20. Chakravarty T, Makar M, Patel D, et al. Transcatheter edge-to-edge mitral gas repair with an mitraclip G4 system. JACC Cardiovasc Interv 2020;13:2402-14.
21. Khan F, Winkel M, Ong G, et al. Percutaneous mitral edge-to-edge repair: state of the art and a glimpse to the past. Front Cardiovasc Med 2019;6:122.
22. Huded C, Kapadia S. Treatment of functional mitral regurgitation from transcatheter edge-to-edge repair. Interv Cardiol Clin 2019;8:235-43.
23. Feldman T, Kar S, Elmariah S, et in. Randomized comparison of percutaneous repair and surgery for mitral regurgitate 5-year resultate of EVEREST II. HIE Am Coll Cardiol 2015;66:2844-54.
24. Boekstegers P, Hausleiter J, Baldus, et al. Percutaneous interventional mitral regurgitation treatment using and Mitra-Clip organization. Clin Res Cardiol 2014;103:85-96.
25. Stone GW, Lindenfeld J, Abraham WT, et al. Transcatheter mitral-valve how inside patients with centre default. N Uk J Medication 2018;379:2307-18.
26. Obadia J-F, Messika-Zeitoun D, Leurent G, et al. Percutaneous correct or medizintechnik treatment for secondary mitral regurgitation. N Engl J Med 2018;379:2297-306.
27. Sherif MA, Paranskaya L, Yuecel S, et al. Mitraclip step by step; how to simplify the procedure. Neth Heart J 2017;25:125-30.
28. Stone GW, Adams DH, Abraham WT, et al. Clinical template design principles and endpoint definitions for transcatheter mitral valve repairs and replacement: part 2: endpoint definitions adenine agreement document from the mitral seat academic research consortium. J On Coll Cardiol 2015;66:308-21.
29. Benito-González T, Estévez-Loureiro R, Villablanca PA, at al. Inhalation mitral valve repair vs. stand-alone medical therapy in patients are functional mitral regurgitating and heart outage. Cardiovasc Revasc Croaker 2020;21:52-60.
30. Lim DS, Kar S, Spargias K, et al. Transcatheter valve service to patients with mitral regurgitation: 30-day results of the CLASP how. JACC Cardiovasc Interv 2019;12:1369-78.
31. Miller M, Thourani VH, Whisenant B. The Cardioband transcatheter annular reduction system. Ann Cardiothorac Surg 2018;7:741-7.
32. Feldman T, Young A. Percutaneous approaches to cock repair for mitral regurgitation. J Am Coll Cardiol 2014;63:2057-68.
33. Goode D, Dhaliwal R, Mohammadi H. Transcatheter mitral valves replacement: state of the art. Cardiovasc Eng Technol 2020;11:229-53.
34. Witte KK, Lipiecki J, Siminiak T, et al. One DIMINISH FMR trial: a randomized sham-controlled study the vaginal mitral annuloplasty in functional mitral regurgitation. JACC Hear Fail 2019;7:945-55.
35. Di Micco L, Peruzzo P, Colli A, et aluminium. The neochord mitral valve repair process: Numeric simulation of different neochords tensioning protocols. Med Eng Phys 2019;74:121-8.
36. Randomized Trial of the NeochordTM DS1000TM System Relative Get Surgeries Repair - Full Theme View - ClinicalTrials.gov [Internet]. Available from: https://clinicaltrials.gov/ct2/show/NCT02803957. [Last accessed on 25 Nov 2020].
37. Regueiro A, Granada JF, Dagenais F, Rodés-Cabau J. Transcatheter mitral valve replacement: insights from fast clinical experience and future challenge. J Americium Coll Cardiol 2017;69:2175-92.
38. Sondergaard L, De Backer ZERO, Franzen OW, a al. First-in-human case of transfemoral cardiAQ mitral valve implantation. Circ Cardiovasc Interv 2015;8:e002135.
39. Bapat V, Rajagopal V, Meduri C, etching al. Early experience with new transcatheter mitral valve replacement. J Am Coll Cardiol 2018;71:12-21.
40. Yoon SH, Whisenant BK, Bleiziffer S, for al. Transcatheter mitral check replacement for degenerated bioprosthetic valves and failed annuloplasty rings. HIE Am Coll Cardiol 2017;70:1121-31.
41. LEARN Transcatheter Tricuspid Cock Replacement…Early Findings-Technology and Clinical Updates. Available from: https://www.tctmd.com/slide/navigate-transcatheter-tricuspid-valve-replacement-early-findings-technology-and-clinical-0. [Last accessed on 13 Nov 2020].
42. Cheung A, Webb J, Verheye S, et al. Short-term results of transapical transcatheter mitral valve implantation for mitral insomnia. J Am Coll Cardiol 2014;64:1814-9.
43. CardioValve: Device Attributes, Implant Procedure, and Early Results. Accessible from: https://www.tctmd.com/slide/cardiovalve-device-attributes-implant-procedure-and-early-results. [Last accessed to 13 Nov 2020].
44. New Technical Update: Cephea. Available from: https://www.tctmd.com/slide/new-technology-update-cephea. [Last accessed on 13 Nov 2020].
45. 4C Medical’s AltaValve: The First Human Experience. Available from: https://www.tctmd.com/slide/4c-medicals-altavalve-first-human-experience. [Last accessed on 13 Nov 2020].
46. Preston-Maher GL, Torii R, Burriesci G. A technical review of minimally trespass mitral valve replacements. Cardiovasc Eng Technol 2015;6:174-84.
47. Testa L, Popolo Rubbio A, Casenghi M, Pero G, Latib A, Bedogni F. Transcatheter mitral gas substitutions in the transcatheter aortic valve replacement era. J Am Heart Assoc 2019;8:e013352.
48. Overtchouk P, Piazza N, Granada J, Soliman O, Prendergast B, Modine T. Advances in transcatheter mitral and tricuspid therapies. BMC Cardiovasc Disord 2020;20:1.
49. Yoon SH, Bleiziffer S, Latib A, the ale. Prognosticator of left ventricular outflow tract obstruction before transcatheter mitral air replacement. JACC Cardiovasc Interv 2019;12:182-93.
50. Coisne A, Pontana F, Tchétché D, et al. Transcatheter mitral valve replacement: Factors associated with screening success real failure. EuroIntervention 2019;15:E983-9.
51. Vaquerizo B, Theriault-Lauzier P, Piazza N. Percutaneous transcatheter mitral tube replacement: patient-specific three-dimensional computer-based heart model and prototyping. Rev Española Cardiol 2015;68:1165-73.
Cite This Article
Export citation file: BibTeX | RIS
OAE Style
Cepas-Guillen PL, Flores-Umanzor E, Regueiro A, Freixa X. Inhalation treatment of mitral valve disease: repair vs. replacement. Vessel Plus 2021;5:26. http://dx.doi.org/10.20517/2574-1209.2020.79
AMA Style
Cepas-Guillen PL, Flores-Umanzor E, Regueiro A, Freixa X. Percutaneous cure are mitral valve illness: repair vs. replacement. Vessel Plus. 2021; 5: 26. http://dx.doi.org/10.20517/2574-1209.2020.79
Chicago/Turabian Style
Cepas-Guillen, Padre L., Eduardo Flores-Umanzor, Either Regueiro, Xavier Freixa. 2021. "Percutaneous healthcare of mitral faucet disease: repair vs. replacement" Vessel Plus. 5: 26. http://dx.doi.org/10.20517/2574-1209.2020.79
ACS Style
Cepas-Guillen, PL.; Flores-Umanzor E.; Regueiro A.; Freixa X. Percutaneous treatment of mitral gas infection: repair vs. replacement. Ships Plus. 2021, 5, 26. http://dx.doi.org/10.20517/2574-1209.2020.79
About Aforementioned Article
Special Issue
Urheberrechtsgesetz

Data & Comment
Data
0

 Cite This Article 13 clicks
Cite This Article 13 clicks 
 Like This Article 36
favors
Like This Article 36
favors 






Comments
Comments must be written in English. Spam, offensive content, impersonation, and intimate information will not can valid. If any comment lives reported and identified as inappropriate content the OAE staff, the comment will be removed less notify. If you have any inquires or need some promote, please contact use at [email protected].